Learn Practical Examples for SOAP, DAP, BIRP, and GIRP Case Notes
Case notes are one of the most important things a social worker writes, and also one of the most inconsistent. Walk into almost any social services organization and you’ll find staff using different formats, different levels of detail, and different ideas about what a good progress note actually looks like. Getting this right matters!
Clear, well-structured social work case notes protect clients, protect practitioners, and make it possible for any team member to pick up a case file and immediately understand what’s happening.
We’ll review the four most widely used case note formats, SOAP, DAP, BIRP, and GIRP, with a real example of each, so you can choose the right approach for your setting and start writing better clinical documentation right away.
What you’ll learn:
- What each case note format covers and when to use it
- A practical case note example for SOAP, DAP, BIRP, and GIRP
- How to choose the right format for your caseload and setting
- Common mistakes that weaken progress notes
- How software can streamline your documentation workflow
Let’s get started
Watch this video:
or
read the guide below.
What Makes a Good Social Work Case Note?
Before diving into format, it helps to understand what all good case notes share, regardless of the structure. Strong social work documentation is timely, written as close to the session as possible. It separates observation from interpretation. It uses clear, plain language rather than vague descriptors like “client seemed fine.” And it includes enough detail that a colleague reading the note cold could understand the client’s current status and next steps without needing to ask questions.
A study published by the National Library of Medicine looked at the benefits of using a standard notes template for patience notes. It found that optimizing note templates saved an average of 2.6 hours per day (23 minutes per client encounter) and improved provider satisfaction.
What Is the SOAP Note Format and When Should You Use It?
SOAP is the most widely recognized case note format across social work, mental health, and clinical settings. It stands for Subjective, Objective, Assessment, and Plan. The structure works well because it forces a clean separation between what the client reports, what the practitioner observes, what it all means clinically, and what happens next.
SOAP notes are a strong choice for clinical environments, hospital social work, and any setting where your notes may be read by medical professionals who are already familiar with the format.
SOAP Note Example:
Subjective: Client reports feeling “overwhelmed and exhausted” since returning to work after a period of medical leave. States she has been having difficulty sleeping and feels disconnected from her coworkers. Denies suicidal ideation.
Objective: Client appeared tired but engaged throughout the session. She made consistent eye contact, spoke at a normal pace, and her affect was congruent with reported mood. No observable signs of acute distress.
Assessment: Client presents with adjustment difficulties following return to work, consistent with situational anxiety and mild depressive symptoms. Current coping strategies appear insufficient for present stressors. No safety concerns identified.
Plan: Introduce cognitive behavioral coping strategies in next session. Provide psychoeducation on sleep hygiene. Schedule follow-up in two weeks. Consider referral for psychiatric evaluation if symptoms worsen.
Example Note from the Case Management Hub Platform
💡All-in-one Case Management Software.
Everything in one place: clients, notes, forms, appointments, reports, and outcomes.
👉 Try it Free - No credit card needed
What Is the DAP Note Format and When Should You Use It?
DAP stands for Data, Assessment, and Plan. It is a condensed version of SOAP that combines the subjective and objective sections into a single Data section. Many practitioners prefer DAP for its speed, making it a practical choice for high-volume caseloads where writing time is limited but consistency still matters.
DAP notes work well in community mental health, outpatient therapy, and nonprofit case management settings where session turnaround is fast.
DAP Note Example:
Data: Client arrived on time and reported ongoing conflict with his landlord that has intensified over the past two weeks. He stated he has been avoiding home when possible and is sleeping at a friend’s place several nights per week. Client appeared anxious, spoke quickly, and had difficulty staying on topic at the start of the session. Settled as the session progressed.
Assessment: Client’s housing instability is exacerbating existing anxiety symptoms. Avoidance behavior is serving as a short-term coping mechanism but is not addressing the underlying conflict. Risk of housing loss assessed as moderate.
Plan: Assist client in drafting a written communication to landlord. Connect with housing mediation resources this week. Reassess housing stability at next session in one week.

👉 Try it Free - Free Case Management System
What Is the BIRP Note Format and When Should You Use It?
BIRP stands for Behavior, Intervention, Response, and Plan. It was designed specifically for behavioral health settings and is particularly popular in substance use treatment, residential programs, and mental health crisis services. The key difference from SOAP and DAP is that BIRP explicitly documents what the practitioner did during the session and how the client responded to that intervention, making it highly useful for demonstrating treatment effectiveness and supporting billing documentation.
BIRP Note Example:
Behavior: Client presented with elevated irritability and reported consuming alcohol three times in the past week following a period of sobriety. He minimized the relapse and expressed frustration with the recovery process, stating “I don’t see the point anymore.”
Intervention: Practitioner used motivational interviewing to explore ambivalence around sobriety. Reflective listening techniques were applied to validate client’s frustration without reinforcing avoidance. Client’s prior reasons for seeking treatment were revisited collaboratively.
Response: Client became more engaged as the session progressed. He identified two personal motivators for continuing recovery and agreed to attend his support group meeting this week. Resistance decreased noticeably by the session’s end.
Plan: Continue motivational interviewing approach in next session. Review support group attendance at follow-up. Reassess relapse triggers and update safety plan.
Example Note from the Case Management Hub Platform
All-in-One Case Management Software
Sign Up Today, Free
No credit card needed!
Do You Have a Team? | ||
Our best all-in-one client and top case management software simplifies everything from client intake and assessments to programs, projects, goals tracking, planning, scheduling, documentation, reporting dashboard, and progress tracking.
What Is the GIRP Note Format and When Should You Use It?
GIRP stands for Goal, Intervention, Response, and Plan. It is the most goal-centered of the four formats, making it an excellent fit for settings that use structured treatment plans tied to measurable client objectives, such as community mental health, rehabilitation services, and programs with funder reporting requirements. Each GIRP note anchors the session directly to a specific treatment goal, which makes it easy to demonstrate progress over time.
GIRP Note Example:
Goal: Client is working toward reducing social isolation by initiating at least one social interaction per week, as identified in her current treatment plan.
Intervention: Practitioner reviewed the client’s progress on her weekly social goal and used solution-focused questioning to explore barriers. Role-playing was used to practice initiating a conversation with a neighbor the client has been avoiding.
Response: Client identified a specific interaction she plans to attempt before the next session and reported feeling “more confident” after the role-play exercise. She acknowledged that her avoidance has been driven by fear of rejection and expressed willingness to challenge this pattern.
Plan: Client will attempt one social initiation before the next session and track the outcome. Practitioner will review results at the following appointment and adjust the goal if the current target has been consistently met.

How Do You Choose the Right Case Note Format?
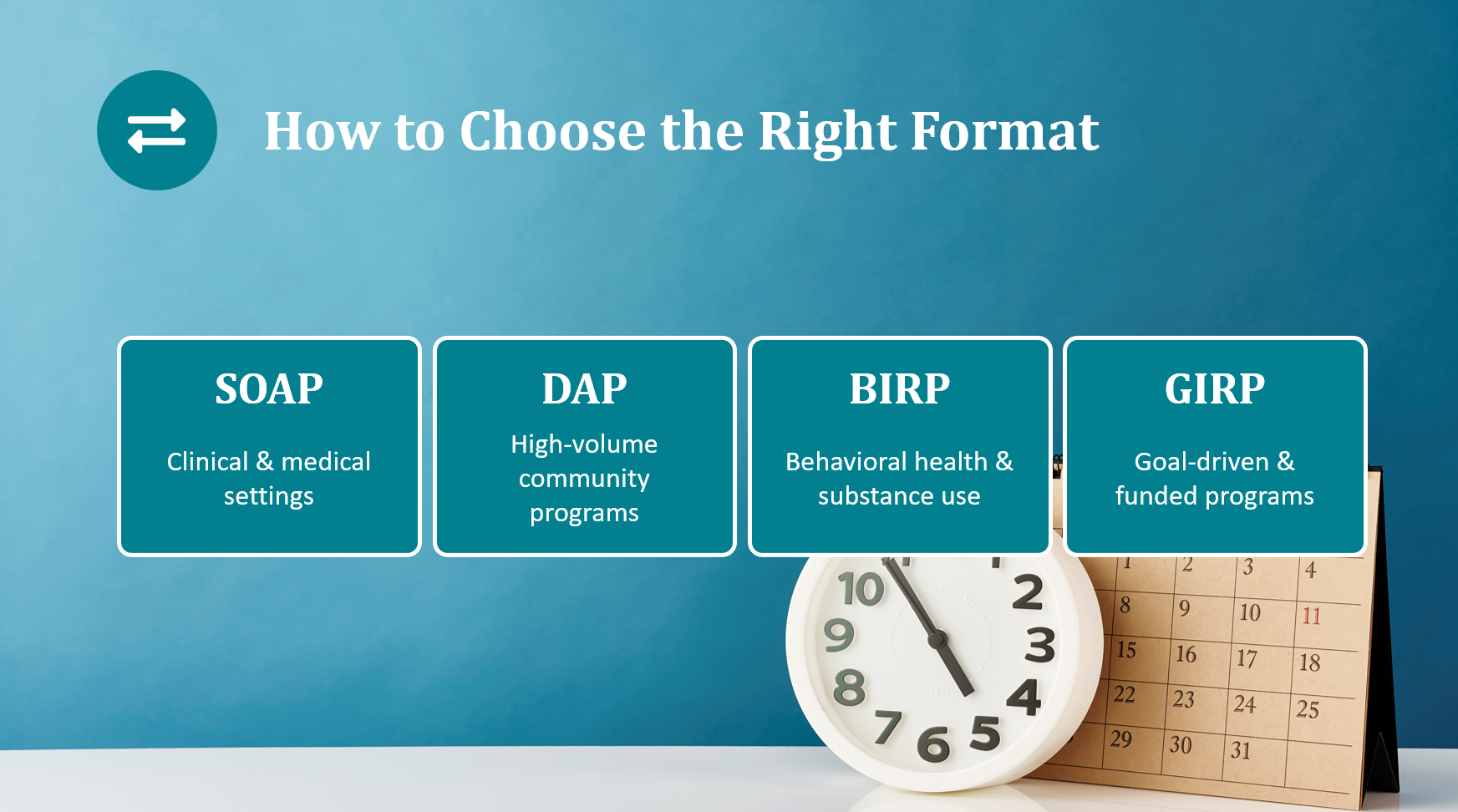
Choosing between SOAP, DAP, BIRP, and GIRP comes down to four practical considerations.
Your setting and audience matter most. Clinical and medical-adjacent environments tend to prefer SOAP. High-volume community programs often gravitate toward DAP for its efficiency. Behavioral health and substance use programs frequently require BIRP because of its documentation of specific interventions. Goal-driven programs with structured treatment plans are a natural fit for GIRP.
Billing and compliance requirements are the second factor. Some payers and funders require documentation of specific interventions and client responses, which makes BIRP or GIRP more appropriate than SOAP or DAP in those contexts.
Caseload size plays a role too. The more clients you are seeing per day, the more you benefit from a streamlined format like DAP that still captures the essentials without requiring four fully developed sections.
Finally, team consistency matters. Whatever format your team chooses, everyone using the same structure makes supervision, audits, and case transfers significantly smoother.
🔥Still using spreadsheets for case management?
Switch to an all-in-one case management platform.
👉 Try it Free - No credit card needed
What Are the Most Common Case Note Mistakes?
Even experienced clinicians fall into the same traps. Vague language is the most common, words like “good session” or “client is doing better” communicate almost nothing to a reader who was not in the room. Delayed documentation introduces memory gaps and undermines the accuracy of the record. Mixing observation with interpretation without labeling which is which muddies the clinical picture. And copying or slightly modifying a previous note rather than writing fresh documentation is both an ethical and legal risk.
The fix for most of these is structural: a consistent format completed promptly after each session, ideally supported by a template that prompts for the right information every time.
How Case Management Software Can Improve Your Documentation
Writing better case notes is easier when your documentation tool is built for the job. Case Management Hub gives social workers, case managers, and clinical teams access to built-in templates for SOAP notes and other progress note formats, all organized within each client’s secure case file. Notes, intake forms, scheduling, goal tracking, and reporting all live in one place, which means less time switching between systems and more time focused on clients. You can explore the full platform and start a free trial at https://www.socialworkportal.com/social-work-case-management-software/
👉 Try this Case Management Software free today
No credit card needed
FAQ: Case Notes for Social Workers
What is the difference between SOAP and DAP notes
SOAP separates client-reported information (Subjective) from practitioner observation (Objective) before moving into Assessment and Plan. DAP combines both into a single Data section, making it faster to write while still capturing the essential clinical picture.
Which case note format is best for behavioral health?
BIRP is widely used in behavioral health because it explicitly documents the intervention the practitioner used and how the client responded, which supports both clinical accountability and billing documentation.
How long should a case note be?
Most case notes run between one and three paragraphs per section. The goal is to capture enough detail that any qualified colleague could understand the client's status and next steps without having to ask questions. Length should serve clarity, not demonstrate effort.
Can you use different case note formats for different clients?
It depends on your agency's policies. Some organizations standardize one format across all cases for consistency. Others allow practitioners to match the format to the client's treatment context, particularly when different programs within the same agency have different documentation requirements.
What should never be left out of a case note?
Every case note should include the date, the client's presenting status, any safety concerns or their absence, what occurred in the session, and clear next steps. Missing any of these weakens the clinical record and increases liability exposure.
Is case notes software worth it for small practices?
Yes. Even solo practitioners or small teams benefit from structured templates, centralized storage, and the ability to retrieve notes quickly during audits, supervision, or client transfers. The time saved on formatting and filing alone tends to offset the cost quickly.
👉 Try it free today - No credit card needed
Note: Content on this website (socialworkportal.com) is copyrighted and protected under applicable copyright laws. Unauthorized reproduction, distribution, or use of any content from the website, without explicit written permission, is strictly prohibited. Read: Terms of Use.
Social Work Portal Disclaimer: Social Work Portal is not a social work agency and we do not refer social workers. This web site is provided for educational and informational purposes only and does not constitute providing medical advice or professional social and healthcare services. The information provided should not be used for diagnosing or treating a health problem or disease, and those seeking personal medical advice should consult with ... Read our full disclaimer here: Social Work Portal Disclaimer.