Mastering Clinical Documentation: What Every Case Manager Needs to Know About SOAP Notes
Poor clinical documentation costs U.S. healthcare organizations an estimated $8.3 billion annually in rework, compliance failures, and care coordination breakdowns.
For case managers, the stakes are even higher, a poorly structured progress note can delay authorizations, compromise continuity of care, and create serious liability exposure.
SOAP notes (Subjective, Objective, Assessment, Plan) remain the gold standard for clinical documentation best practices precisely because they impose a consistent, defensible structure on a complex clinical process.
Let’s get started
Watch this video:
or
read the guide below.
What We Will Cover
- What a SOAP note is and why the format exists
- How to write each of the four SOAP sections correctly
- The most common documentation mistakes that create compliance risk
- How SOAP notes compare to DAP and BIRP formats
- Best practices for care plan documentation and clinical note quality
- Real-world examples and a section-by-section breakdown
- How digital health documentation tools support SOAP note consistency
- Frequently asked questions from case managers and healthcare teams
Everything in one place: clients, notes, forms, appointments, reports, and outcomes. 👉 Try it Free - No credit card needed💡All-in-one Case Management Software.
What Is a SOAP Note and Why the Format Matters
The SOAP note format was developed by Dr. Lawrence Weed in the 1960s as part of the Problem-Oriented Medical Record system. Decades later, it endures because it mirrors the natural clinical reasoning process, gather patient input, observe measurable data, analyze findings, then act.
Every section has a distinct purpose, and when each is executed well, the result is a note that communicates clearly across disciplines, supports billing accuracy, and withstands regulatory scrutiny.
For case managers working in complex, multi-provider environments, this structure is especially valuable. SOAP note charting in care coordination creates a shared clinical language that reduces miscommunication between physicians, social workers, insurers, and community-based providers.
The Four Components at a Glance
| SOAP Component | What It Captures | Common Errors |
| Subjective (S) | Patient’s reported symptoms, concerns, history | Mixing in clinician interpretation |
| Objective (O) | Measurable, observable clinical data | Including unverified patient statements |
| Assessment (A) | Clinical judgment, diagnosis, status | Being vague or omitting clinical reasoning |
| Plan (P) | Next steps, referrals, follow-up actions | Listing actions without rationale |
👉 Try it Free - Free Case Management System
How to Write the Subjective Section
The Subjective section captures the patient’s own words and perspective. It is not a place for clinician interpretation, if the patient says “my pain is a 7 out of 10 and started after I lifted something heavy last week,” that language belongs in S verbatim or paraphrased without editorializing.
How to write a subjective section in a SOAP note correctly means documenting the chief complaint, history of present illness, relevant past medical/social/family history, and any changes since the last encounter.
Strong subjective sections also include the patient’s functional status, support system observations, and self-reported barriers to care, all of which are critical inputs for case management progress notes that drive actionable care planning. Avoid the common mistake of blending subjective reports with your own clinical interpretation; that analysis belongs in Assessment.
Writing the Objective Section: Data Only
Objective data in clinical documentation refers to anything measurable, observable, or verifiable without relying on patient self-report. This includes vital signs, lab values, diagnostic results, medication reconciliation data, functional assessments (e.g., Katz ADL scores), and direct behavioral observations made during the encounter.
For case managers, objective data may also include third-party reports from care team members, verified attendance records for treatment programs, or documented functional limitations from occupational therapy evaluations. The key discipline here: if you cannot independently verify it, it does not belong in O.
SOAP Note Documentation: Objective Section Checklist
| Data Type | Examples | Documentation Tip |
| Vital signs | BP 142/88, HR 76, O2 sat 97% | Include date/time of measurement |
| Lab/diagnostic results | HbA1c 8.2%, chest X-ray findings | Reference report date and ordering provider |
| Functional assessments | Katz ADL score 4/6 | Specify tool used and who administered it |
| Behavioral observations | Alert, oriented x3; flat affect noted | Use neutral, descriptive language |
| Third-party reports | PT notes: ambulating 50 feet independently | Cite source and date |
What Goes in the Assessment Section of a SOAP Note
What goes in the assessment section of a SOAP note is the question clinicians most frequently get wrong. Assessment is not a restatement of the subjective complaint or a list of diagnoses, it is your clinical synthesis. This is where you connect the dots: given what the patient reported (S) and what you measured (O), what is your professional judgment about their current status, progress toward goals, and clinical trajectory?
Effective Assessment sections in SOAP notes for social workers and case managers include a status update on active diagnoses, barriers to care plan adherence, risk stratification, and response to current interventions. The Assessment is where your clinical expertise becomes visible in the record, and it is the section most scrutinized during audits and utilization reviews.
Do You Have a Team? Our best all-in-one client and top case management software simplifies everything from client intake and assessments to programs, projects, goals tracking, planning, scheduling, documentation, reporting dashboard, and progress tracking.All-in-One Case Management Software
Sign Up Today, Free
No credit card needed!
Building an Actionable Plan Section
The Plan section should leave no ambiguity about what happens next. Every action item, medication adjustment, referral, follow-up appointment, patient education task, or escalation, should be documented with enough specificity that a colleague covering for you could execute it without a phone call. This is where care plan documentation standards intersect directly with operational efficiency.
SOAP note examples for case managers consistently show that high-quality Plan sections include: the responsible party for each action, a target timeframe, and a clear clinical rationale. Weak Plan sections list generic actions (“follow up as needed”) that create accountability gaps and undermine documentation compliance in healthcare.

SOAP Notes vs. Other Clinical Note Formats
Not every setting uses SOAP. Understanding where SOAP excels, and where alternatives like DAP (Data, Assessment, Plan) or BIRP (Behavior, Intervention, Response, Plan) are preferred, helps case managers advocate for the right documentation standard in their organization.
SOAP Note vs. DAP Note: Key Differences
| Feature | SOAP Note | DAP Note | BIRP Note |
| Separates S from O | ✅ Yes | ❌ Combined as “Data” | ❌ No |
| Best for | Medical/ multidisciplinary | Behavioral health | Mental health therapy |
| Audit defensibility | Very high | Moderate | Moderate |
| Supports billing codes | Strong alignment | Moderate | Strong for therapy |
| Care coordination clarity | Excellent | Good | Limited |
For mental health SOAP note guidelines, many organizations now use hybrid formats, but the four-part SOAP structure remains the most defensible and widely recognized across payers and accreditation bodies.
Common SOAP Note Mistakes That Undermine Quality
Understanding how to improve clinical note quality starts with recognizing the patterns that erode documentation value. The most frequent errors seen across case management teams include:
- Crossing section boundaries: Documenting clinical opinion in the Objective section, or measurable data in the Assessment
- Vague Plan language: “Continue current plan” with no specifics about what the current plan entails
- Missing timestamps or encounter context: Notes that cannot be reliably associated with a specific encounter date
- Failure to link Assessment to Plan: A diagnosis or risk identified in A with no corresponding action in P
- Copy-forward documentation: Cloning previous notes without updating for the current encounter, a significant compliance risk
Effective patient progress notes depend on discipline and consistent structure. Organizations that invest in SOAP note training for healthcare teams see measurable improvements in audit outcomes, authorization approval rates, and care coordination efficiency within 90 days.
People Also Ask
What is the purpose of a SOAP note in case management?
SOAP notes in case management create a structured, legally defensible record of clinical encounters that supports continuity of care across multiple providers. They document the patient’s current status, clinical reasoning, and next steps in a format that payers, auditors, and care team members can quickly interpret, making them essential for authorization support, care transitions, and outcomes tracking.
How long should a SOAP note be?
There is no universal length requirement, but effective SOAP notes prioritize specificity over volume. A well-written note may be as concise as 200–400 words if each section is precise and complete. Length should be driven by clinical complexity, not habit, longer notes filled with vague or repeated language are a documentation liability, not an asset.
Can SOAP notes be used for mental health documentation?
Yes, and mental health SOAP note guidelines from major behavioral health accreditation bodies, including CARF and The Joint Commission, recognize SOAP as an acceptable and often preferred format. The Subjective section is particularly valuable in mental health contexts for capturing the patient’s self-reported mood, thought content, and functional concerns in their own words.
What is the difference between subjective and objective in a SOAP note?
Subjective data is what the patient reports, symptoms, concerns, and history that cannot be independently verified by the clinician. Objective data is what the clinician can observe, measure, or verify through testing and third-party sources. Keeping these rigorously separated is the most common discipline challenge in SOAP documentation and the most important for audit defensibility.
Are SOAP notes required by law?
SOAP notes are not mandated by a single federal law, but documentation compliance in healthcare regulations, including CMS Conditions of Participation, HIPAA, and state licensure requirements, mandate that clinical documentation be accurate, complete, dated, and authored by a qualified provider. SOAP format meets these requirements and is widely accepted across payers and accreditation standards.
How do SOAP notes support care coordination?
SOAP note charting in care coordination creates a consistent clinical language that reduces handoff errors, supports transitions of care, and enables multidisciplinary teams to quickly assess patient status without duplicating assessments. When all team members document in SOAP format, the patient record becomes a reliable, real-time view of care progress.
Switch to an all-in-one case management platform. 👉 Try it Free - No credit card needed🔥Still using spreadsheets for case management?
How Case Management Hub Can Help
Inconsistent SOAP documentation is one of the most common, and most correctable, drivers of authorization denials, compliance findings, and care coordination failures. Case Management Hub is built specifically for the workflows case managers and care coordination teams navigate daily, providing structured documentation tools that enforce SOAP format integrity without slowing clinical staff down.
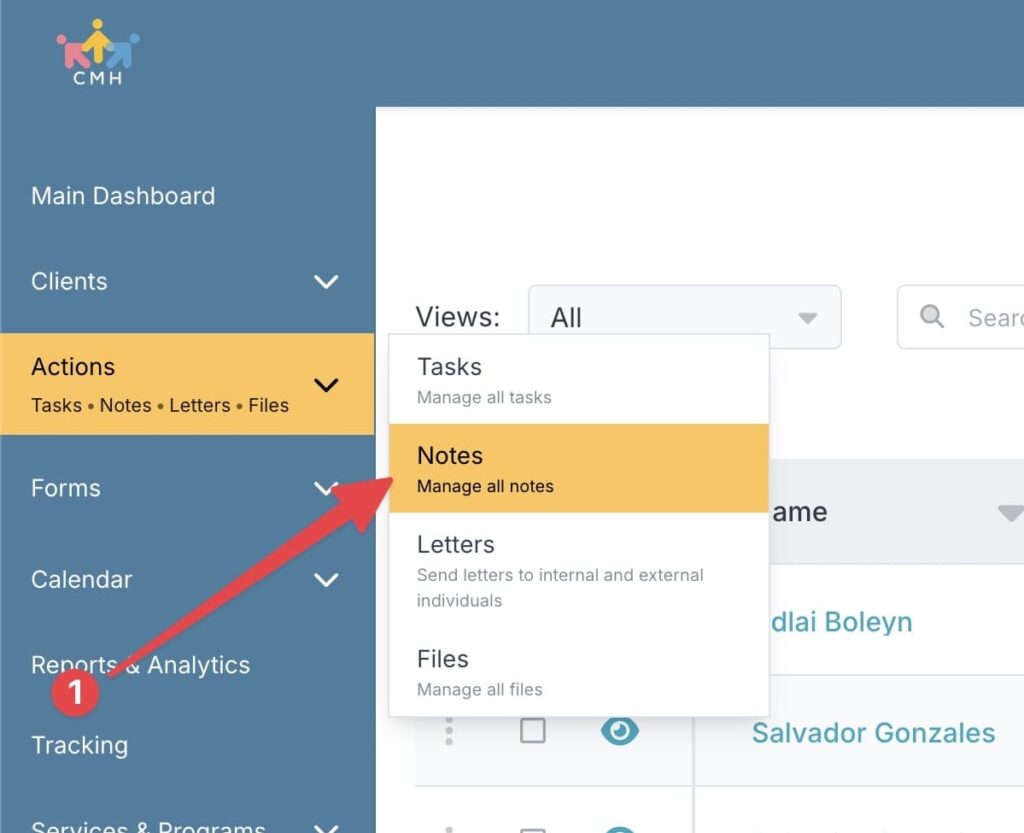
To create a SOAP note in Case Management Hub:
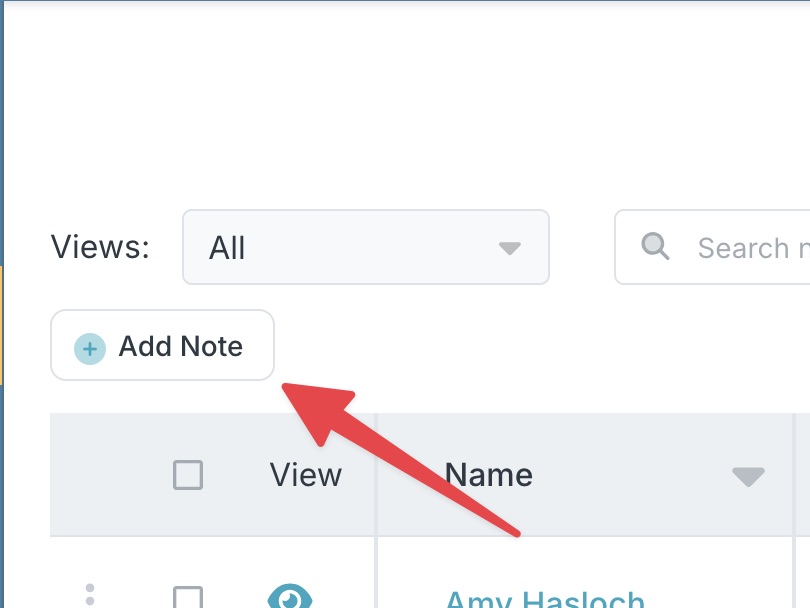
Step 1:
Navigate to the Notes module from the sidebar and click Add Note
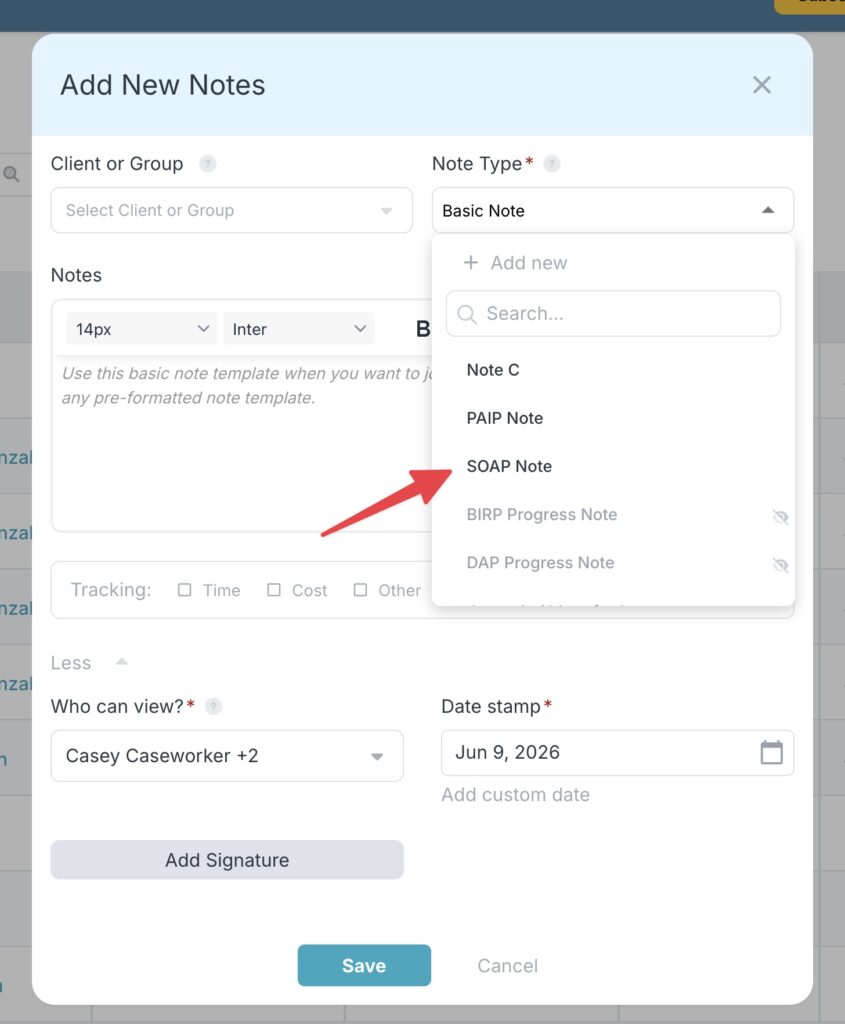
Step 2:
From the note type dropdown select the SOAP note template
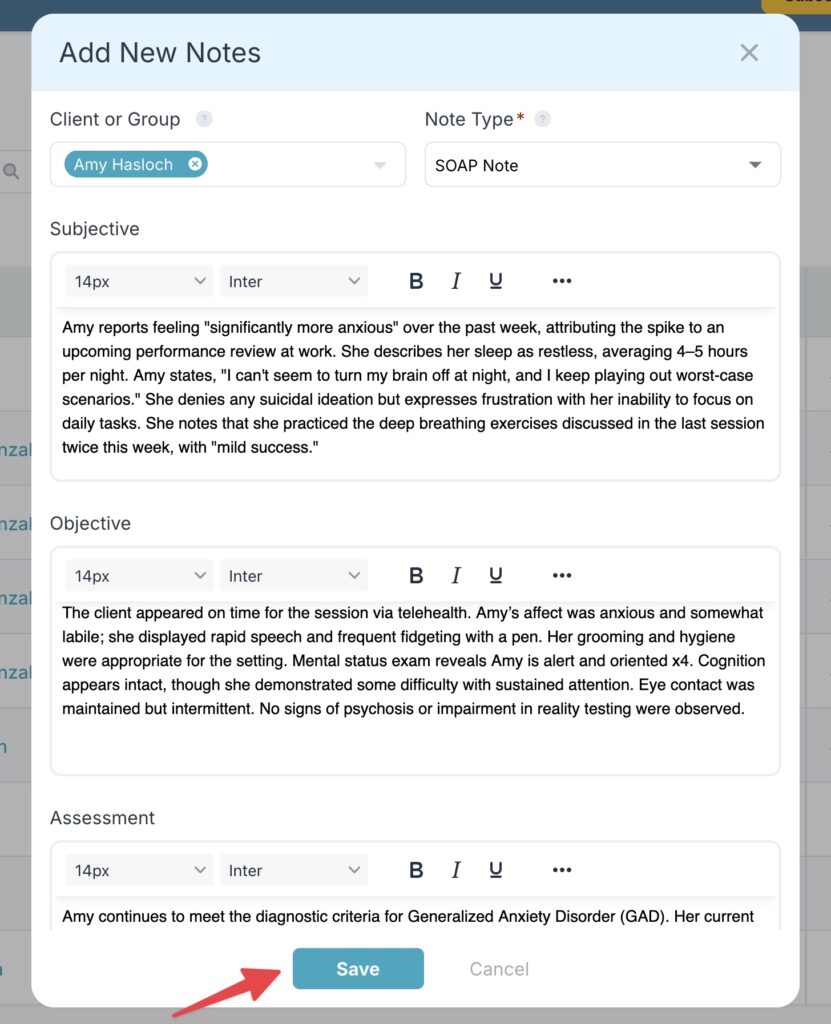
Step 3:
Add your note details to the four sections of the SOAP note, select the client, and then click save.
Step 4:
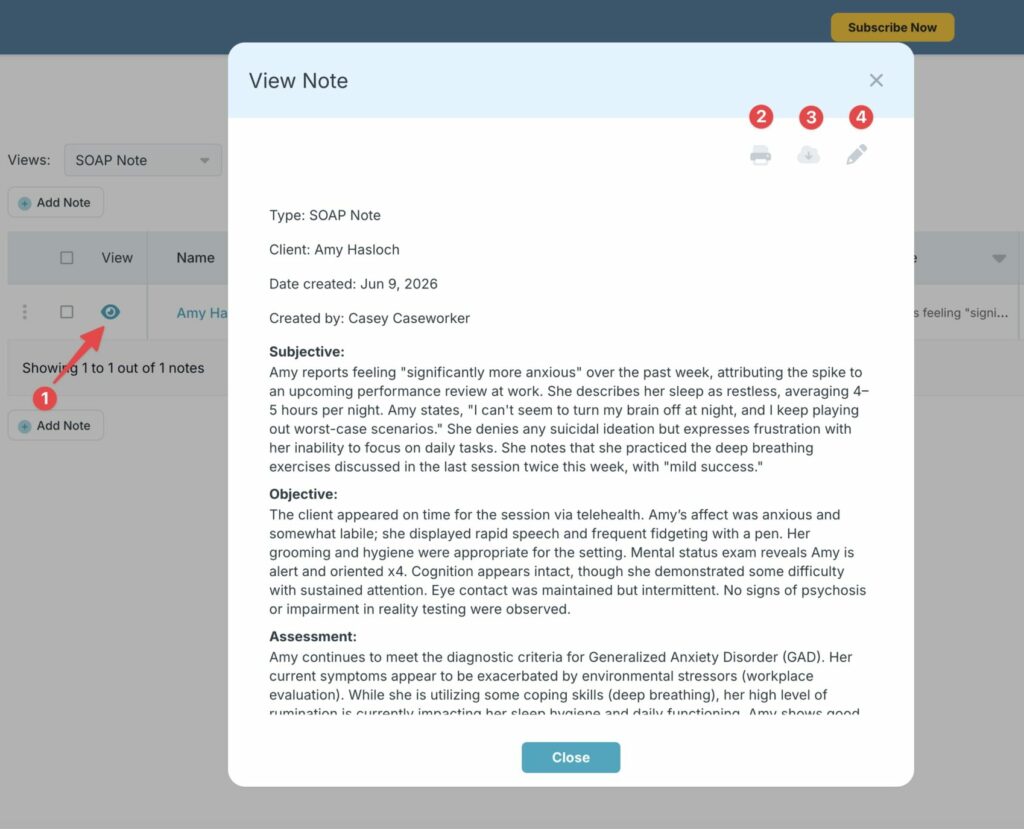
View, search and filter all of your client notes, including the SOAP notes in one place.
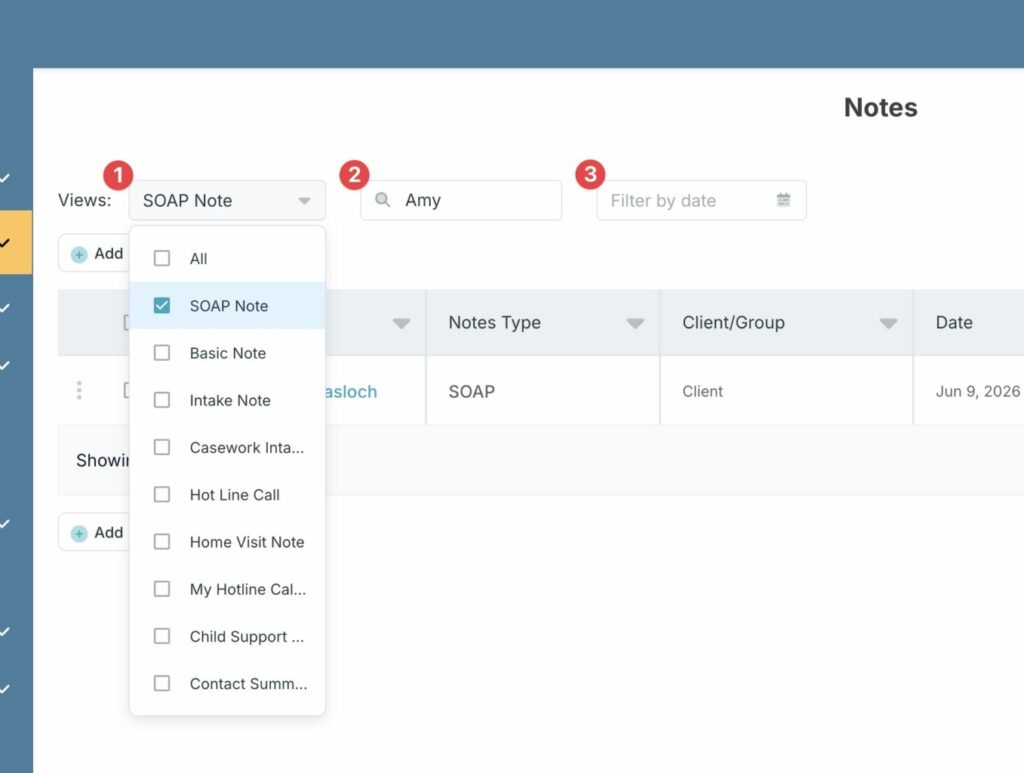
Step 5:
Click the eye icon to view or edit the details of the note
If you’re interested in improving you’re teams SOAP notes documentation, then check out our free 21-day trial today (no credit card needed).
👉 Try it Free today - No credit card needed
Frequently Asked Questions about SOAP notes
The Assessment section requires you to make a clinical argument, not just summarize what you observed. Start by identifying the core clinical problem or impression, then connect it explicitly to evidence from your Subjective and Objective sections. For example, rather than writing client struggling, write: client demonstrates moderate psychosocial risk consistent with recent housing instability, caregiver burden, and declining PHQ-9 scores over the past 30 days. Specificity is your credibility. Reference validated tools, trend data, and treatment milestones to give the Assessment clinical weight.
In community health, SOAP notes often emphasize social determinants of health alongside clinical indicators. A strong Subjective section might document transportation barriers, food insecurity disclosures, or caregiver stress. The Objective section could include home visit observations, functional assessment results, or collateral reports from community health workers. The Assessment should address both clinical and social risk factors, and the Plan should include community-based referrals, resource connections, and cross-agency coordination steps, with clear timelines and responsible parties named for each action item.
A compliant SOAP note template should include clearly labeled fields for each of the four components, mandatory fields for date, provider name, and encounter type, and prompts that prevent common errors such as mixing subjective and objective content. Templates used in digital health documentation tools should also include fields for risk screening documentation, telehealth-specific information when applicable, and signature/attestation fields that satisfy payer and accreditation requirements. Off-the-shelf templates without clinical validation may create compliance gaps.
Payers, including Medicare, Medicaid, and commercial insurers, review clinical documentation to determine whether billed services are medically necessary and appropriately coded. A SOAP note that lacks a clear Assessment tied to a billable diagnosis, or a Plan that doesn't correspond to the billed intervention, can trigger claim denial or audit. Strong subjective objective assessment plan documentation creates a direct, auditable link between the clinical encounter and the billing code, protecting revenue and reducing compliance exposure.
Inadequate SOAP note documentation creates legal exposure in multiple directions. In malpractice cases, incomplete or internally inconsistent notes suggest inadequate care. In fraud and abuse investigations, copied notes or vague Plans raise questions about whether documented services were actually delivered. SOAP note compliance and legal documentation standards require that notes be completed contemporaneously, reflect the actual encounter, be signed by the credentialed provider, and be corrected through addendum rather than deletion if errors occur.
Yes. Non-clinical case managers, including those working in housing, workforce development, or social services, can adapt the SOAP framework by replacing clinical terminology with role-appropriate language. The Subjective section captures the client's self-reported situation and goals. The Objective section documents observable facts and assessment tool results. The Assessment synthesizes barriers and strengths. The Plan outlines agreed-upon next steps. The underlying logic of separating reported information from observed data, and both from professional judgment, is universally applicable and strengthens documentation quality across all case management disciplines.How do I write the Assessment section without sounding vague?
What are SOAP note examples for case managers working in community health settings?
Is there a SOAP note template that meets clinical and compliance standards?
How does SOAP note documentation affect billing and reimbursement?
What are the legal risks of poor SOAP note documentation?
Can SOAP notes be adapted for non-clinical case management roles?
👉 Try it free today - No credit card needed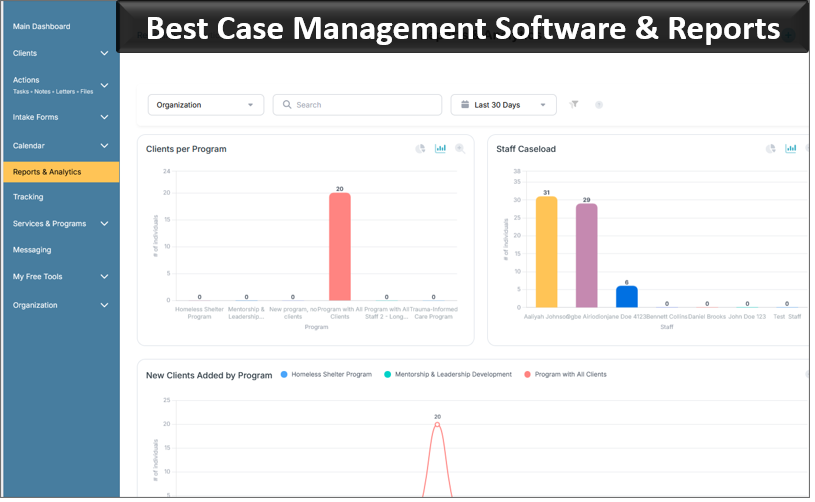
Note: Content on this website (socialworkportal.com) is copyrighted and protected under applicable copyright laws. Unauthorized reproduction, distribution, or use of any content from the website, without explicit written permission, is strictly prohibited. Read: Terms of Use.
Social Work Portal Disclaimer: Social Work Portal is not a social work agency and we do not refer social workers. This web site is provided for educational and informational purposes only and does not constitute providing medical advice or professional social and healthcare services. The information provided should not be used for diagnosing or treating a health problem or disease, and those seeking personal medical advice should consult with ... Read our full disclaimer here: Social Work Portal Disclaimer.